.webp)
If you've been diagnosed with COPD, you may have left your doctor's office with a name for your condition but not much clarity on what's actually happening in your lungs. COPD, chronic obstructive pulmonary disease, is an umbrella term. Underneath it sit two distinct conditions: emphysema and chronic bronchitis. They often coexist, but they affect the lungs differently, tend to produce different symptom patterns, and understanding the distinction can help make sense of what you're experiencing day to day.
First, a common question worth addressing: COPD is not contagious. It is not an infection that spreads between people. What causes COPD is long-term damage to the airways and lung tissue, most commonly from cigarette smoking, but also from prolonged exposure to air pollution, chemical fumes, dust, and in some cases, genetic factors like alpha-1 antitrypsin deficiency. What causes COPD besides smoking is increasingly recognized as a significant contributor, particularly in people who have never smoked but have spent years in polluted or occupationally hazardous environments.
What Is Emphysema?
Emphysema affects the tiny air sacs at the end of the airways called alveoli, where oxygen passes into the bloodstream. In emphysema, the walls between these air sacs are progressively destroyed, creating larger, less efficient spaces that can't exchange oxygen effectively. The lungs also lose their natural elasticity, making it harder to fully exhale. Air gets trapped.
The dominant symptom of emphysema is shortness of breath, or breathlessness, which tends to be most pronounced during activity.
In the early stages of COPD with a primarily emphysematous pattern, people often notice they can't do things they used to without becoming winded. Wheezing and COPD of this type can also coincide, particularly during exertion or when oxygen levels drop during activity. The cough associated with emphysema tends to be mild or even absent. What's more prominent is the progressive breathlessness and the effort it takes to push air out.
People with emphysema often breathe with pursed lips, an instinctive adaptation that creates back-pressure in the airways and helps keep them open during exhalation. Over time, the chest can take on a rounded, barrel-like appearance as the lungs hyperinflate to compensate for trapped air.
What Is Chronic Bronchitis?
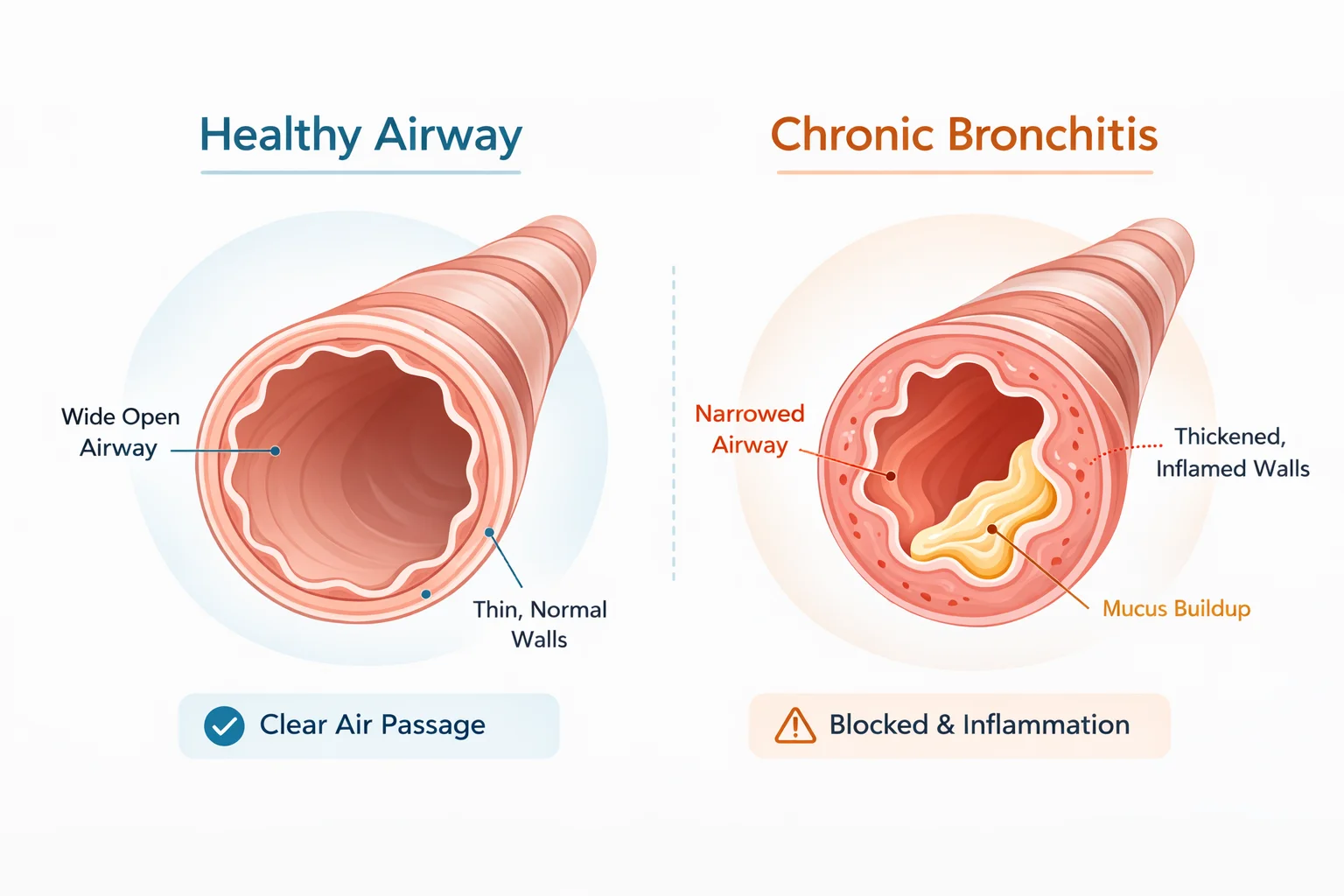
Chronic bronchitis affects the airways themselves rather than the air sacs. The bronchial tubes become chronically inflamed, and the mucus-producing glands within them go into overdrive. The result is persistent mucus buildup and a productive cough, meaning a cough that regularly brings up phlegm.
By clinical definition, chronic bronchitis involves a cough with mucus production on most days for at least three months of the year, for two or more consecutive years. That's not just a winter cough that lingers; it's a sustained, recurring pattern.
Shortness of breath is also present in chronic bronchitis, but the predominant day-to-day experience tends to center on the COPD cough, the feeling of congestion, and the effort of clearing the airways. Lung sounds in chronic bronchitis often include wheezing and crackling, sounds produced by air moving through narrowed, mucus-filled airways. These COPD lung sounds are one of the clearest indicators clinicians use to distinguish bronchitic from emphysematous patterns during examination.
Why Most People Have Both
In practice, emphysema and chronic bronchitis rarely exist in pure isolation. Most people with COPD have features of both, in varying proportions. A long-term smoker might develop significant destruction of the air sacs alongside chronic airway inflammation, experiencing both persistent breathlessness and a productive daily cough.
What COPD causes in any individual depends on a combination of factors: smoking history, genetics, environmental exposures, and how long the disease has been progressing.
Research also shows that a significant subset of COPD patients exhibit what's called an allergic phenotype, elevated sensitivity to environmental triggers like pollen and pollution, which can influence how symptoms present regardless of which structural pattern dominates.
This overlap is one reason COPD symptoms can feel so inconsistent. On a high-pollution day, airways already narrowed by chronic bronchitis become more reactive. After a poor night's sleep, the breathlessness of emphysema feels more pronounced. A COPD flare-up rarely has a single cause; it tends to reflect several factors loading up at once. COPD home monitoring of breathing patterns and daily habits over time can help reveal what combinations tend to precede difficult days for any individual.
Why the Distinction Still Matters
Knowing which pattern is more dominant in your COPD isn't just academic; it can inform conversations with your healthcare provider about what to watch for and how your symptoms tend to behave. The COPD treatment landscape has also evolved to recognize these differences: certain medications, including roflumilast, are indicated specifically for the chronic bronchitis phenotype with frequent exacerbations, rather than for COPD broadly.
The NHLBI and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) both emphasize that COPD management works best when it's tailored to the individual, their symptom pattern, their exacerbation history, and the factors that seem to influence their breathing day to day.
If you're unsure which pattern fits your experience, it's worth raising with your doctor. And if you're tracking your breathing patterns over time, paying attention to whether breathlessness or cough and mucus tends to dominate, and what conditions seem to coincide with each, can produce genuinely useful information to bring to that conversation.

When You Have Both, the Picture Gets Complicated
If your COPD involves features of both emphysema and chronic bronchitis, as it does for most people, the day-to-day experience can feel hard to read. Is today's breathlessness the emphysematous side reacting to poor sleep? Is the heavier cough tied to air quality, activity, or something else entirely? When two distinct patterns overlap, single observations rarely tell you much.
Respire LYF is designed for people with asthma and COPD. It automatically connects the factors that tend to coincide with breathing changes across your day, from how you slept and what the air quality was, to how often you coughed and whether your inhaler was on schedule, so you can start to see which combinations tend to precede your harder days, whether breathlessness or cough tends to dominate, and what your pattern actually looks like over time. It doesn't diagnose or interpret your symptoms. But it gives you something more useful than memory to bring to your next conversation with your doctor.
This article is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult your healthcare provider about your symptoms and care.